  Let’s paint a picture. Saturday is the day. You have been training for this event for months. You are passionate about your health and habits contributing to a personal goal. You have realized gains in strength, surpassed personal best records and have the edge going into the last week prior to your event. Someone recommends that you receive massage to help you prevent injury and control your mental game as you make final preparations. You make an appointment for a massage for the Friday night before the event. Your therapist employs, what they call, deep tissue massage in order to break up adhesions. Your therapist administers general or full body massage as a means of stress management. They even stretch every muscle in your body at the end of the session. You get off of the table feeling better than you have in quite some time. You drink the prescribed water to “flush out toxins that were squeezed out by the massage” (BS). Pain that you thought you could never rise above has left your body. You drive home with a drunken smile doing 40mph in a 55mph zone. You go to bed early.
Saturday. Your alarm goes off. You feel like you have been hit by a garbage truck. Joints are hurting. You have DOMS, delayed onset muscle soreness. Movement is bothersome if not painful. Coffee doesn’t do its normal trick. You want to crawl back in bed. You are the victim of a train wreck a mere 100 feet from its final destination. For the moment, all gains are lost. You need two days of recovery. Massage as an integral part of training can factor in that competitive edge many are looking for. Also true, massage can inhibit the same desired results. Yes, goal oriented and outcome-based massage therapy sessions impact an athlete’s ability to perform better and recover quicker. But, the one flippant session immediately before or after an event really does not weigh in when it comes to desired results. In fact, without certain key elements adhered to, massage can cause gains in training to be lost come game time or create a reality in which such gains are not as possible to begin with. Desired results, optimal and measurable results, warrant that massage therapy be responsible if it is to be an integral part of training. Responsible massage therapy
Let’s consider another, actual, scenario. One of my athletes comes in for his weekly sessions. He’s a sprinter. His sessions are timed at the end of practice at the end of the week. Before getting on the table he announces that instead of coming out of practice, he will be going to practice after his massage session. That changes everything about the session. Instead of a one hour, general or full body session targeting tight hamstrings followed by stretches with the goal of lengthening stride, we change to a 30-minute session that only hits large muscles groups. The length of the session is not the only thing changed. Pace, rhythm, drag, duration, depth, technique and the outcome itself are also changed. Rather than working towards flexibility and range of motion, we target the nervous system in order to stimulate. Rather than inhibiting muscle tightness in one group of muscles, which can be a workout in and of itself, we activate large muscle groups. Rather than inducing recovery, we prepare both the muscular and nervous system for action. Instead of going into practice with a parasympathetic nervous system reaction, calm and relaxed, which would have been the case, he went into practice with his nervous system in a sympathetic state, prepared for action. We could have cancelled the appointment. We did not because of his current health and vitality, his ability to respond to the stress of a massage session. If he had been a weekend warrior I would have just rescheduled the session for afterwards to induce recovery. You should be thinking:
1. Now I’m confused. Rightly so. Misinformed or ill-informed professionals working outside of their professional scope of practice will do more damage than good especially when it comes to educating the general public as to the benefits of massage for athletes. Even reading articles online will serve to add to the confusion. So, be careful that WHAT you read is supported properly. Ask your therapist for information supported by clinical trial studies and peer reviewed journals. Here is a good place to start, the massage profession’s only open-source, peer-reviewed academic journal, the International Journal of Therapeutic Massage & Bodywork. As an example: HERE. Another from AMTA describes the benefits of massage for headaches: HERE. There is evidence supporting the benefits of massage as part of an athletes training to include injury prevention and injury recovery. Look at the references listed in Massage For Those Who Exercise. See that they ARE listed is the point. There is a difference in a topically oriented professional opinion and a study that presents objective findings followed by implications for further study. 2. Okay. Why should I risk it? Why should I bother? “Individuals who participate in exercise and athletic programs who seek enhanced performance, improved conditioning, faster recovery, injury prevention, and assistance in maintaining peek fitness can benefit from massage therapy given by professional massage therapists working within their scope of practice.” That’s why. Above and Below is taken from the last article mentioned and the references are also found in same article. Again: Here. Research has shown that in relation to exercise and athletic participation massage can:
3. What type of massage do I need? What can I expect as far as therapy goals and modalities used in a session? A Licensed Massage Therapist that has training working with athletes will take a lot of information into consideration in designing a treatment plan for you. The two of you will agree upon all aspects of proposed treatment plan. It’s called an informed consent. The type of massage and treatment goals established as well as the modalities used in a session will be informed by data collected at the onset. Aside from a health intake form, your LMT will ask the following questions:
Your LMT will conduct various visual, palpable and functional assessments in order to determine if it is safe to work on you or whether you need to see a different professional. These assessments will also inform your therapist as to which tissue needs attention and which type of therapy. Types of massage, modalities, will match the goals that you establish as they produce physiologic outcomes conducive to the same. In general terms, and depending on your current health and needs, your treatment plan will indicate whether muscles or nervous system is to be targeted or a combination of both. Yet, even within those parameters, a decision to inhibit or stimulate is to be made depending upon your recent and planned activity level. (If you just ran a Half Marathon you don’t want to wait a week to receive work. If you’re running a Half tomorrow you don’t want to receive any work. If it is 30 minutes to start time you can receive a 10 min warm up as long as it is stimulating and not taxing. If you just ran a 5k and your idea of hydration is Miller Lite …No) There is a lot to consider. But a clear treatment plan should be encouraging as you can see how it fits into the grand scheme, your fitness activity and goals. So, a typical treatment plan for my sprinter is as follows: Weekly
Pre event warm up
Within 2 hours post event IF last event of the day
I do not list modalities on a menu board for selection. “I think I’ll try some myofascial release today followed by Active Isolated Stretching and finish with an Essentric Pin and Stretch”. No. It starts with a goal. The therapist chooses which tool to remove from his/her tool belt in order to match physiologic outcomes with a goal. The therapist also only carries tools in his/her tool belt that they are comfortable using. So, focus on the goal. Choose a seasoned and knowledgeable therapist, not a modality (fad technique) As far as goals, you most likely already have one in mind being that you’re considering such therapy. It can be as simple as:
Or just pick from the list of benefits noted earlier, 4. When is the optimal time for receiving massage therapy as a structural and planned component of training? As you can see by now, timing is important. Your recent and future activity dictates when.
5. Which therapist do I need? Well, if you live near me… www.bobbylewislmt.com Outside of NW Georgia? Check the websites for AMTA and ABMP for a listing of therapist in your area. They should have listed specialties per therapist as well. Sports Massage. Neuromuscular Therapy. Orthopedic Massage. Your local runners club or college athletic department may have a referral. Chiropractors and LMTs often work together. If I were in the market for a therapist I would ask fellow athletes. You want a seasoned therapist that has a following. May be harder to get on the books so once you are able, schedule the whole year out in advance and ask for a discount. If the therapist tells you to drink water to flush out the lactic acid and other toxins that they broke loose during the massage… pay your bill. don’t tip. walk away. Keep looking.
0 Comments
Let me tell ya lil story bout a messed up thumb... As a Massage Therapist, having my hands hurting constantly with fingers locking in pain, unable to work, is not conducive to making a living...paying bills, or even being somewhat effective at work. I struggled with trigger tendons for a year. I kept working and tried various therapies and was prepared to take a several month break to have surgery. But no... Trigger Tendons can be painful. They can often just be annoying or even a cool trick to show friends. The anatomy involved is, of course, tendons, but as there is inflammation on the tendon as it passes through a sheath or crosses a pulley at the joint. It can lock. The release of this locked tendon is visible with a snapping twitch, painful or not. I still have one trigger tendon that has never been painful. And it does not go away. I ignore it except to show it off at parties. I have had four other trigger tendons that brought tears to my eyes and made me articulate my feelings about said pain using colorful metaphors and choice expletives. , sometimes during treatment with a client on the table.
I sought help first from an orthopedic doctor. I received injections which took away my pain 100%, until I went back to work a week later. Pain and inflammation returned w a vengeance, this time in an additional digit. I then sought help from my massage therapists, Mariam Samha and Marlene Turner. Both were able to give me some relief as they were thorough in treating all the way up to my elbow. Mariam performed myofascial release and pin and stretch methods to include each digit and short muscle of the hand as well as longer muscle in the forearm. Marlene then applied a new treatment technology using a combination of frequency-emitting wearable sticker discs, ANF therapy. I realized some relief from both but it was only temporary. I see their work as valid, yet the intensity and measure of reoccurring debilitating pain had me willing to undergo surgery.
But then a funny thing happened. This guy proposes to my daughter. My baby girl will be married come May 2019. Other than joy and happiness for both of them, I also experience fear and sadness. "I got to get my butt in better shape so as to be present at the wedding...to give my daughter away." I knew what I must do. Lifestyle changes that include diet and exercise. As I started I was intentional about eliminating all foods and beverages that cause inflammation. So sad. I also added items that combat inflammation. So, hello healthy food, goodbye processed food, sugar, alcohol. "Hey, my hands dont hurt anymore." What? I got rid of my trigger tendons even while increasing the volume of my massage practice by
It took 4 weeks to restore the strength and health of my hands and fingers without taking a break from work. Im at 90%. My therapists could have done more over time, but the root cause was an inflammatory state due to what I was consuming. Input equals Output. Ive done Adkins when Keto wasn't cool. I discovered Ketogenic research 7 years before it became a fad. Ive done Primal and Paleo. Ive lost 800 pounds over the last 15 years. Minus 50 plus 60, minus 70 plus 80, minus 20 plus 25 ...etc. Im not saying Ive arrived and have the answers to anything. Dont follow me. Im just saying my hands don't hurt. I lost weight. Im going to a wedding. Im giving my daughter away. Oh, bacon is its own food group. 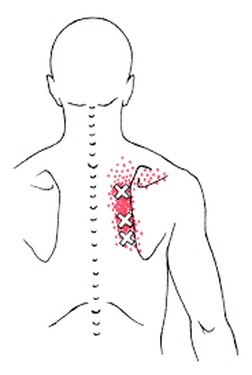 As is often the case I see clients with similar issues during a short period of time: identical headaches, same rotator cuff issue, tennis elbow...etc. The past two weeks Ive encountered several presenting with the same chief complaint, upper back pain. They usually have the same story to tell as well. "It's right between my shoulder blades but more so on the right side. I've been rolling a ball on that spot and it gets better for a day, but then it comes right back." Rolling a ball on that spot, equal to foam rolling or a therapist that only works on that painful spot, will help for a brief time. Consider that the cause of pain is coming from somewhere else. If the pain continues to return then obviously a more thorough treatment is warranted. If your Massage Therapist, Chiropractor, PT, AT isolates the area of pain in treatment without investigating as to the reason for the onset and progression of pain, much can be missed. I know many professionals ask questions about repetition, prolonged shortening, posture and ergonomics. But, too often, the simple relationship among antagonistic muscle groups, those that act opposite of each other, are not considered. MANY issues with the upper back and too many issues with rotator cuff impingement are a direct result of Upper Crossed Syndrome, medially rotated shoulders and forward head posture. While there may not be an obvious postural distortion, as with athletes and bodybuilders, it still involves the dominance of one group of muscles and the inhibition or lengthening of the opposing group of muscles. As with the cases of upper back pain I'm referring to, and with athletes and bodybuilders, the pecs, shoulders and lats are tight and weak leaving the traps and rhomboids long and weak. Having tight muscles is not a sign or guarantee of optimal strength. A short and tight muscle is not as strong as it could be. A long muscle, being pulled by the opposite group of muscles, is also not as strong as it could be. Some muscles, when stressed, shorten. Other muscles, when stressed, lengthen. This describes perfectly the relationship between the muscle groups Ive identified. Pectoralis Major, Anterior Deltoid, Latissimus Dorsis, Teres Major, and Subscapularis are all medial rotators of the shoulder. Serratus Anterior is an abductor of the scapula, pulling it around the ribcage. When they are stressed they shorten giving rise to medial rotation and Upper Crossed Syndrome. The opposite group of muscles, Posterior Deltoid, Infraspinatus, Teres Minor, Rhomboids, and Trapezius are being pulled along into a lengthened position, allowing Upper Crossed Syndrome. Restoring this balance between the groups of muscles is crucial to resolving issues of pain and dysfunction. It is crucial for optimal strength and athletic performance. How do I address it? I tell my athlete to "take a break from the gym. We must normalize the tissue first, relieve pain and reduce inflammation. Instead of working to further shorten the culprit group of muscles, I will work on them to lengthen them and then you must do the appropriate stretches for the same. If I only work on the painful area it is going to continue to come back. If we rest and lengthen the one group of muscles it will take the tension off of the long and weak group of muscles, allowing them to regroup. When you go back to the gym, double the amount of lateral rotation of the shoulder and retraction of the scapula compared to that of pushing and pulling with the dominate group. In other words, work your post delt, infra and rhomboids 2:1 to that of pecs, lats...etc. Therapy on the shortened group of muscles involves a lot of gliding, pin and stretch, and trigger point work immediately followed by stretching. After Ive worked the pecs and other medial rotators, I have them stand and stretch. I have them test the area of pain. Often it is already diminished without having worked on the painful area yet. I still work on the painful spot between the scapula., but only after Ive addressed the culprit. As has been reported, individuals are experiencing greater relief. The ones that quit the gym for a week get more results in and out of the gym. 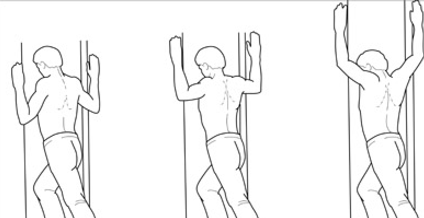 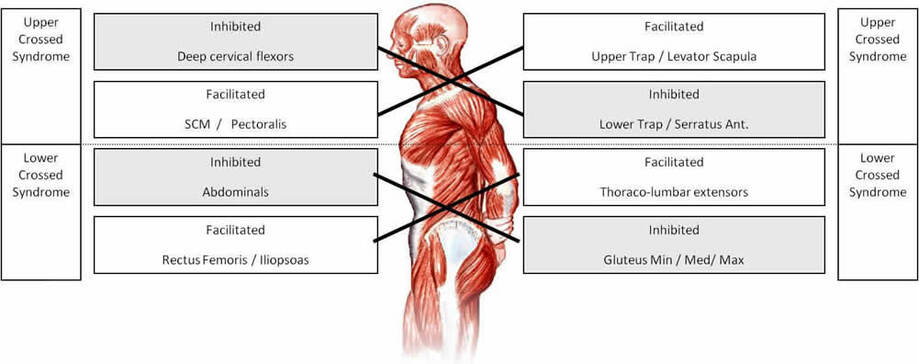
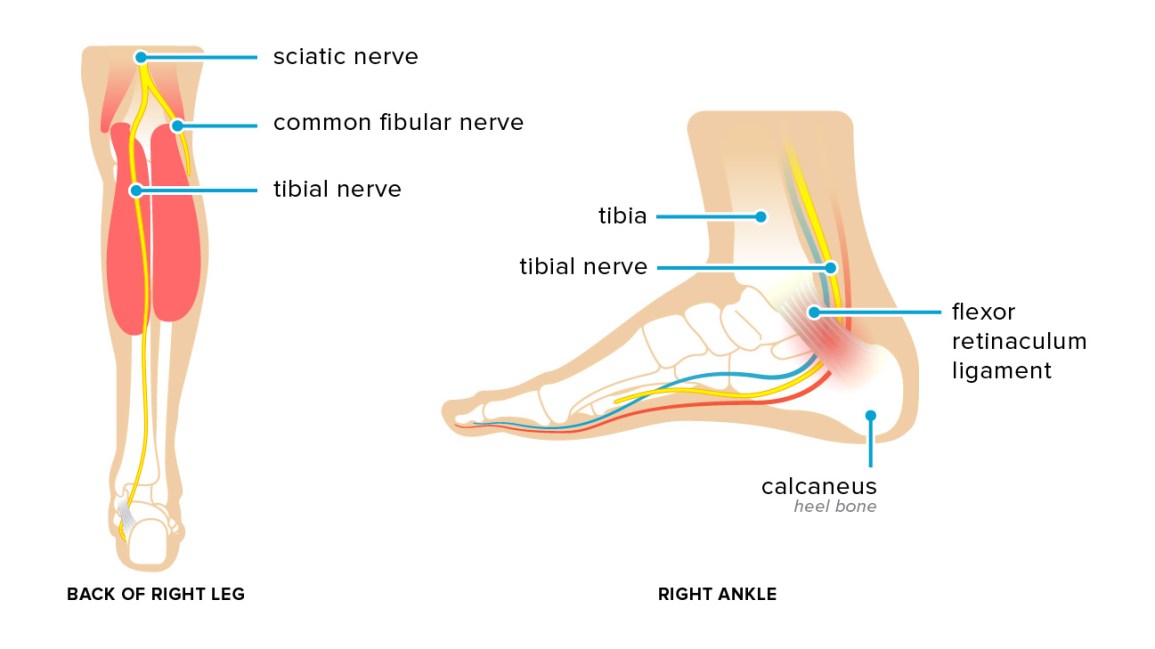
2/4/2019 0 Comments Tarsal Tunnel Syndrome
Just as we have the carpal bones of our wrist that form a tunnel in which artery and nerve and tendons may become impinged and cause pain and numbness, the tarsal bones of the ankle along with a retinaculum, connective tissue, can also impinge the tibial nerve. Tarsal Tunnel Syndrome is no where near as common as carpal tunnel syndrome, but it can be very debilitating to those that endure it
4/2/2015 0 Comments Daytona Bike Week Yes, I have a brother.
The following conversation via email: JE: Gotta testymoanial fer ya.....I can shake your hand but I can't turn a door knob. Rode the Harley to Daytona and back. Started getting cramps at the neck shoulder junction. Neck / shoulder stretches dint do nuthin. By accident I found that stretching the white side of my forearm cleared it all up. Who'd a thunk it! Now fer a ?. Got back and went to work. Found that I could squezze big things but small motor function was shot. Weak as a kitten. Couldn't screw a screw, turn a knob, could barely write, couldn't even take the gas cap off. As last week wore on, the weakness has faded somewhat, but I still have trouble time to time. I've stretched everything I can find but the prob persists. 'Sup widdat? Sister Laura (also a therapist) says my flexors are #$%&$, but to ask you cause yer a dang jeanyus. Bobby: Laura, I agree with flexors. Especially if it’s both hands. If only right hand look at extensors for throttle...…wrist extensors. Supinator and digitorum below lat condyle. If only right look at radial nerve irritation …anywhere from scalene to wrist. Include stretching the forearm flexors and neck at the same time. Possible diaphragm from riding so long causin scalene to work overtime breathing. Possible that vibration caused ulnar nerve irritation. Possible that the forward flexed posture of riding served to develop trigger points in your medial rotators, thus referring to your hand. ... reach behind you like your getting something out of the back seat. Put your palm flat on the wall. Turn to the opposite side and look over opposite shoulder as if to look in your back pocket. Yeah, that felt good dinnit? Hold that stretch for several seconds, come out of it then do it again. Repeat until fine motor function returns. JE: Wow. You were right Laura, he are a geenyus. Just lookit all them fancy words. I'll bet he even knows what they mean too. But that stretchy thing pulled all kinda thangs in my fingers forearm and neck. Dunno how I missed all of them, but I know whar they at now by golly! Ya'll rekun doing that afore and after each ride will handle thangs? Or more oftener? Bobby: Stretch before you ride. Stretch after you ride. If you take breaks, stretch while on break. If your not planning on taking breaks, then TAKE a break to stretch. JE: Sounds doable. If ridin by myself the breaks are when I feel like it. In a gaggle of bikes, the breaks are when the lead guy breaks or the smallest bike runs outta gas. For some reason that always seems to be way after I'm ready to break. Oh well, thats life in a society I guess. Druther be a nomad searching for some place to pillage and wimmen to dominate. You gotta git a bike so we can go do $*%@. Thanks Bro Feel better already! Ken, a fireman, came to me with plantar fasciitis, a painful inflammatory condition that affects the bottom of the foot and the inside of the heel. Walking, especially in the mornings, was excruciating. To Ken, the pain was so debilitating that he couldn’t complete his drills and training. Without successful treatment, Ken was facing a temporary layoff from a job he loved!
I used ice massage on Ken’s foot to numb the pain and reduce the swelling. I utilized a tool that produced friction on his heel and stimulated the tissue to repair itself. Friction stimulates collagen regeneration. I found several trigger pointsand very tender points in his calf muscles. The treatment was uncomfortable, but he was determined to do whatever it took to take care of the problem and to keep his job. I also taught Ken how to stretch his calf muscles properly. After a second visit to satisfy myself that Ken knew exactly what to do to maintain his progress, Ken was happily finished with my services. When I saw Ken at church later the same week, he was walking without a limp! Ken was able to complete his training and drills. Although he has to keep doing the stretches to stay pain-free, he is once again fit and ready to do whatever the job requires. No splint. No meds. No surgery. 9/18/2014 0 Comments Why Am I Having Headaches? Headaches are very common among a significant percentage of people. Most treatments include medication. Most treatments attack the symptom and not the cause.
I developed an expertise in headachesearly in my pain management practice. I truly believe that if I cannot get rid of a headache that there is something a little more serious that may be wrong, and I will refer to your doctor quickly. Honestly, 99%, meaning there was 1 out of 100 that stumped me, was caused by muscle tension. This muscle tension was caused by bad posture, prolonged shortening or overuse/misuse at work, play, sleep, ...…etc. Typically, my line of questioning begins with: 1. Where does it hurt? 2. What type of work do you do? 3. What position do you sleep in? 4. How do you sit at your desk, couch, car…, ...etc. 5. What do you spend most of your time doing? The following Case Study is a good example of finding a simple cure for a headache. A Kindergarten Teacher, Linda, who was in her early 20’s came in for treatment for debilitating daily headaches. She appeared to be stressed. (No kidding.) Fidgety. Pacing. Linda had been trying different medications for several months. The meds would take the edge off of debilitating pain, but did not keep the headaches away. We designed a treatment plan to target the nervous system and promote relaxation so that she could sleep better. The plan also included targeting specific muscles that are generally associated with her typical headache. During treatment, we discovered trigger pointsin her neck and shoulders that mimicked the headache pain. Figuring out why the muscles had shortened in the first place was a mystery. My never-fail questions failed. Driving posture? Sleeping position? Work activities? So far, we were hitting a dead-end. Linda is a teacher, and not just any teacher, she's a Kindergarten teacher. What could Linda be doing teaching kindergarteners that would shorten neck and shoulder muscles? Is there anything unusual that Linda would do during her day that other teachers might not do? One of my greatest joys is finding out the root cause of pain. It’s almost a euphoric feeling to know that I’'m on the right track, as ideas begin to take shape. “ "When you talk to your children one-on-one and you want to look them in the eye, do you kneel on the floor or do you bend forward with your hand on your knees and look up at their face?"” I asked. Her answer, "I bend forward and move my head so that I am looking up"?” The ah-ha moment! We lengthened the muscles, which had shortened with the awkward position. Linda started taking a knee when she talked to her kids. The headaches disappeared. No more need for medication. And Linda did not have to come back to see me. Oh, and she started sleeping better. Good productive sleep took care of her stressed appearance, fidgety and pacing. 2/6/2012 0 Comments Carpal Tunnel Syndrome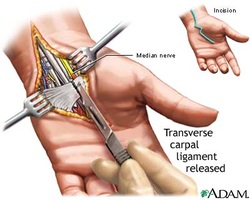
Case Study #1: A mechanic, John, is scheduled for carpal tunnel surgery in a few weeks. I found trigger points in lats, back muscle, and subscapularis, rotator cuff, that refers the identical pain to his wrist. The supervising physician agreed that I had found the source of pain, but also believed that John had suffered with the symptoms for so long that surgery was still a must. This does happen. Still, carpal tunnel surgery, more often than not, only treats the symptoms.
Case Study #2: A teacher, Mandy, is scheduled for surgery in a few weeks. I found trigger points in her upper traps, shoulder, that refers the identical pain to her wrist. Mandy condition developed from writing overhead on a white board in her classroom. I treated her three times. The pain left! Mandy’s doctor cancelled the surgery. Case Study #3 A massage therapist, Autumn, had carpal tunnel surgery 4 months prior to seeing me. The searing pain had returned with the same intensity. Working as a massage therapist contributed to the strain in her neck and schoulders.I found trigger points in her shoulder and neck that sent the identical pain to her wrist. I treated her twice. The pain disappeared. Case Study #4: A Typist, Beth, was scheduled for surgery in a few weeks. I found trigger points in her neck that sent the identical pain to her wrist. I treated her twice. The Dr. cancelled the surgery. Case Study #5: A Sonographer , Jessi, has pain in her wrist. She was told by her family doctor to see a specialist. When she came to see me, I found trigger points in her neck, shoulder and back that sent the identical pain to her wrist. Her pain disappeared. I am still waiting to hear the end of the story. 2/3/2012 0 Comments Chronic Cough, Post SurgeryPenny had undergone surgery for an aneurysm five years earlier. Post surgery, she developed a constant cough. Every 30 seconds to a minute she had to cough. Her surgeon was inclined to believe that the surgery caused nerve damage. Penny did not want to undergo another surgery. She spent the following years coughing every minute of the day. This interrupted all aspects of her life, sleep, work, home. When she entered my clinic, and before we were introduced, I could actually see the tightness in her neck muscles. She explained her history and chief complaint. We started work promptly. Without delay we found trigger points in several muscles of her neck that caused the feeling of needing to cough. Her cough was not productive, it was just a tickle in her throat that made it feel like she needed to cough. We determined that the position that she had to be in on the operation table was the weightiest factor in the shortening of these neck muscles as well as the consequent development of trigger points.  We never completely got rid of her cough but did reduce the intensity and frequency by 90%. Her happiest report was that she was able to eat Doritos again without having to cough. Her testimony is below.
I cannot say enough of what Neuromuscular Therapy has done for me in the short time I have been in this treatment. I had surgery in 1997 due to an aneurysm in the back of my left eye. I had some kind of trauma to my throat or a slight stroke about three months after. Since, and for nine years now, I have been enduring a constant need to cough. Over the years the cough had become so severe that my physical health was affected. The nerves and muscles were so tight in my neck and in so much stress that I often felt like I would probably have a major stroke in my throat. I felt I was a hopeless case. It is amazing how much my cough has improved with this therapy. The stress I had in my neck and throat is at a level that has given me a new positive outlook. I have also learned therapy I can do at home that helps in maintaining my cough and the stress in my throat. I have been impressed how knowledgeable the therapists are in dealing with my particular situation. They listen to me, change the type of therapy as needed or indicated and it is working. I know I will have to continue these treatments to keep me from regressing back to where I was. I just wished more people knew about this kind of therapy so they could see positive results as I have. It has certainly changed my life. A young man, 30, made an appointment as a last chance in finding relief from his back pain before surgery. As a teen he hurt his back in a fall. Physical therapy taught him some coping skills at best. As a steel worker in his 20’s, his back continued to hurt him. He later took an office job. His pain got worse. Surgery was his recommended course of action. Due to the location of his pain, straight line across his low back and straight line across his lower thoracics, mid back, I went directly to two specific trigger point locations on his abdominals. He worked out a lot and put a significant amount of time working on his abs. He did have a 6-pack. This was another indicator that I might find the culprit in hisabdominal muscles. 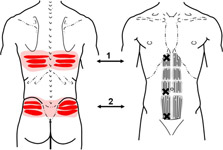 “It’s my back that hurts. Why are you working on my stomach”, he questioned with disbelief. I replied, “If I work exactly where you hurt, 75% of the time I am working in the wrong place. It may feel good or right for me to work on the location of pain but I am more than likely NOT working on the cause of the pain. Plus all of the sitting you do followed by all the ab work you do in the gym, I think these muscles are shortened and may have trigger pointsthat can refer to the back.” It took less than 2 minutes to find the first trigger point in his rectus abdominus muscle that referred pain to his mid back. Working that trigger point referred pain straight through to his back and felt like “a rod going all the way through, just like it does when it hurts real bad”. The pain left. Working on his lower abdominals elicited the same response for his low back, again “like a rod going straight through just like it does when it hurts”. Again, his pain was alleviated. I also performed a pin and stretch on his deeper psoas muscle, a primary hip flexor, which mimicked even more familiar pain. Again, “that worked, I don’t hurt”. I taught him some stretches to do in order to maintain his pain free status. I also showed him how to find these trigger points on his abs so that he could treat himself when he hurts. He walked out without any pain. NO SURGERY NO REPEAT VISITS. 1/30/2012 0 Comments Words of BlessingA dear friend that I treat for debilitating back pain shared thoughts, realizations, about the words we speak, or don't speak to ourselves. I was blessed. I have a lot to learn concerning blessing myself with my words. Enjoy.
Friend: "Spiritually, I'm learning to bless my back the same way I bless Stormy, our crippled goat. I give her extra love and attention because she's the wounded one...just like Jesus going to the 1 and leaving the 99. I don't know when I started doing this,but, in my heart, I've seen my back as the enemy instead of the wounded one. I had Stormy in my lap in the pasture one day and was telling her how special she is and how happy I am that she was born and came into our lives and how we didn't mind at all the special care, that we loved her best. In that moment, I had an epiphany that there was nothing in anything I said to her that I felt or said about myself and my back. It stunned me. So, I've changed the rudder of this ship to bless the wounded parts and when I'm exercising to be visualizing a healing back and muscles that work and a back that is estoring. I wish you'd write an article on it. Being around so many injured people, I'm not alone in this kind of thinking. We even label body parts as "the bad knee and the good knee". We slip into that thinking without even realizing it." I may write an article on it one day. But I don't think I can say it any better! 1/29/2012 0 Comments You Cant Fix My ShoulderA team of therapists and I were working on several teachers at a local high school for Teacher Appreciation Day. A football coach, Mike, took a seat in front of me. I asked him if he had any trouble spots or pain. Mike admitted to significant shoulder pain.
“But you can’t fix it. It’s been going on for three years. I haven’t been able to throw a football since then”. Mike was quick to tell me. I love a challenge. I immediately put my thumb on a specific rotator cuffmuscle. “Is this your pain”? I asked, but his reaction was extreme enough that he didn’t need to use words. “”YES! You’re on a nerve or something”! “ “No, Coach, that’s a trigger point in your lateral rotators. It’s the muscle that puts the breaks on when you follow through throwing a football”. He was skeptical. “I still don’t think you can fix it, but go ahead”. Five minutes later he sat up and showed me how far he could raise his arm, as if to throw a football. “I can only reach this high”. Coach lifted his arm just so. “I can’t take it this high”, he started to demonstrate. His arm floated on up as if there was never a problem. “Hey, wait a minute! I can… Look at this… and it doesn’t hurt”! he practically sputtered. I smiled knowing this was one of the reasons I do what I do. Giving a football coach back the ability to throw a football again is what it’s all about. Coach comes to the clinic now. We released his shoulder pain so that he can continue to do what he loves. “Now, if you can fix my back pain, I’ll give you a million dollars”! he said on one of his visits, still sure that he had me stumped. Thirty minutes later, after I released trigger points in the muscles of his low back and glutes, a sheepish coach asked, “Will you settle for a steak dinner”? I love what I do. BTW...If you're reading this, Coach, I never did get that steak dinner! 1/26/2012 0 Comments Olympian and Ironmannyrr.org/races/pro/interview/2007/krige102907.asp
Krige Schabort was an avid surfer growing up in Cape Town, South Africa. He also enjoyed rugby and squash, and become active in the South African military as a young man. In 1987, during a Cold War battle with Angola, a bomb from a Russian fighter plane hit Schabort. He nearly died, and was saved by an adrenaline shot to his heart. When he woke up days later, he learned that both of his legs and one finger had been amputated. As a disabled athlete, Schabort broke South African swim records and competed in wheelchair basketball. But it was in his first wheelchair race in 1988 that Schabort found his passion. Schabort moved to Cedartown, Georgia, with his wife in 1997. Now sponsored by wheelchair manufacturer Invacare, Schabort has repeatedly won the Cleveland,LaSalle Bank Chicago, Pittsburgh, Detroit, and Columbus Marathons, among others. He placed third in the marathon at the 1992 Paralympic Games in Barcelona with a 1:30.23 and second in Sydney in 2000 with a 1:29.28. In 2004, he was accepted into the Honolulu Marathon’s Hall of Fame, after winning for the seventh year in a row. Schabort has also racked up many 10K victories, and holds the world record for 10 miles with a time of 35:18. During the 2002 New York City Marathon, Schabort set a new course record with a time of 1:38.27. The next year, he won the race again and broke his own record with a 1:32.19 (since broken). At 44, (2007) Schabort is still a top contender amongst a stacked class of racers… Addendum by Bobby Lewis, LMT, Corrective Bodywork shared with permission I met Krige when he first came to my clinic seeking help with his training and performance in the upcoming Paralympics Games. He was in training for the Paralympics Games. As a hand cycling athlete, he wanted to increase his ability to contract his abdominals as well as improve his range of motion with his shoulders. He had specific groin pain as well. We designed a treatment plan to include myofascial release at the hip and through his abs in order to lengthen the muscles that had been shortened from repetitive use. On the first visit of several, we discovered trigger points in his abs that referred pain to his groin as well as to his foot! Yes, his foot! The trigger point referred to what is called a “phantom pain.” When these trigger points were released, his abdominal muscles lengthened. The range of motion in his shoulders increased so he would have great “reach and pull.” Krige reported greater strength during daily training. He went on to the Olympics and competed very well. Two years later Krige returned to my clinic again for help in strengthening and training for an upcoming triathlon. He had limitations in his over-hand free-style stroke which limited his ability to turn his head to breathe during the swimming competition. He had pain in his neck on one side and headaches. The problem was rooted in the medial rotators of his shoulders. His lats had also shortened. With myofascial release, neuromuscular therapy and MET stretches, we lengthend his Lats. We did the same treatment on the neck muscles that rotated his head to the opposite side. After his first visit, Krige went directly to the pool to train. He returned the same week for more treatment and was happy to report that he had taken a full minute off of his best time! Kriege attributed this to his ability to reach further with the one arm and the ability to turn his head without limitation or pain, in order to breathe. Each week thereafter he reported a continual drop off of his best time. Krige is a determined human and a remarkable athlete. He knows firsthand the value of supplementing his training with manual therapy and giving himself the winning edge in competition. It has been an honor to be a part of this championship athlete’s journey. 1/26/2012 0 Comments Golfer's DilemmaI recently worked on a 60 year old gentleman, daily golfer, complaining of pain in his ribs, shoulder, elbow, forearm, hand and index finger. His index finger bothered him the most as it constantly popped (trigger tendon) and affected his grip and swing.
I began working on the larger muscle groups that affected his ribs. Working across his back to his side I found fascial adhesions, very tender, that restricted his backswing and follow through. Releasing theses adhesions on his larger back muscle,Latissimus Dorsi, and abdomen, External Oblique, corrected this for him. A specific stretch before and after a day of golf maintained his improved swing and follow through. While working this area I found trigger points that referred pain to his elbow, hand and wrist. This didn’t totally ease his pain but it did diminish it. So, I looked at hisrotator cuff muscles on the same side. Again I found trigger points in hisInfraspinatus muscle that referred pain to his shoulder and his elbow, also alleviating his pain. I then worked down his arm to his biceps, and other elbow flexors. You guessed it. The trigger point discovered there referred pain to the rest of his wrist and finger. He was 75% better after the first treatment. He returned the same week. We did the same treatments. We added specific treatment on the forearm, his wrist and finger extensors. No more pain. I taught him some stretches to do before he teed off and upon completing 18-27 holes (walking of course). He is able to maintain his improved grip, swing and game with the warm up stretches and finishing stretches. He didn’t have to quit playing. NO DRUGS ! NO CARPAL TUNNEL SURGERY ! My wife received a call from a friend requesting that I help her with her back pain. I agreed to see her. I learned that she suffered from debilitating back pain in her mid back for the last eight months. Bending to pick something up off of the floor, twisting, and deep breathing caused pain. Secondary complaint was her neck pain. She could not rotate her head very far without pain.
She received long term treatment for her back pain to no avail. Actually, her back pain worsened after treatment. I palpated her mid back in the location that she indicated. It was tender. But, since she had been receiving treatment for so long in that immediate area, I decided to look for the culprit elsewhere. I turned her over on her back and began looking for trigger points in herabdominal muscles and diaphragm. It was almost immediate that we located 4 different trigger points that referred pain to the exact location in her back. It was intense. After relieving those trigger points I looked a little higher on her ribs for cardiac arrhythmia trigger points that usually mimic panic attacks. Sure enough, they were there. They cause a feeling of nervousness and trembling that is typical of such trigger points. I worked on her for 20 minutes. She stood up, tested it by bending over to pick up her shoe. No pain. She twisted above the waist. No pain. She took a deep breath. No pain. I questioned about repetitive activity that could put those abdominal muscles in such a shortened and twisted positioned that could be inhibiting her diaphragm from contracting enabling her to breathe properly. When I put her in the specific shortened position as these muscles indicated she immediately knew that it was her hobby of quilting that was to blame. Actually her posture while quilting was to blame. Leaned forward, shoulders rounded and head forward all inhibited her breathing. She was forced to breathe using her chest and neck muscles more than her diaphragm. She had developed several trigger points in her abdominals and diaphragm that referred to her back. The problem was not in her back. She is correcting her posture and breathing pattern with the homework that I gave her to do. She may need a second appointment. But, then again, she may not. Thank you SO much. I feel so much better tonight, and I’m making a concerted effort to keep my posture correct – I have to ‘unlearn’ some bad posture habits. You gave me a lot of good advice.Blessings, Michele 1/11/2012 0 Comments First Post!
Start blogging by creating a new post. You can edit or delete me by clicking under the comments. You can also customize your sidebar by dragging in elements from the top bar.
|
CategoriesAll Carpal Tunnel Chronic Cough Golf Low Back Pain Mid Back Pain Olympic Athlete Post Surgery Shoulder Thoughts Archives
September 2019
Bobby LewisNeuromuscular Therapist 
|





 RSS Feed
RSS Feed
